


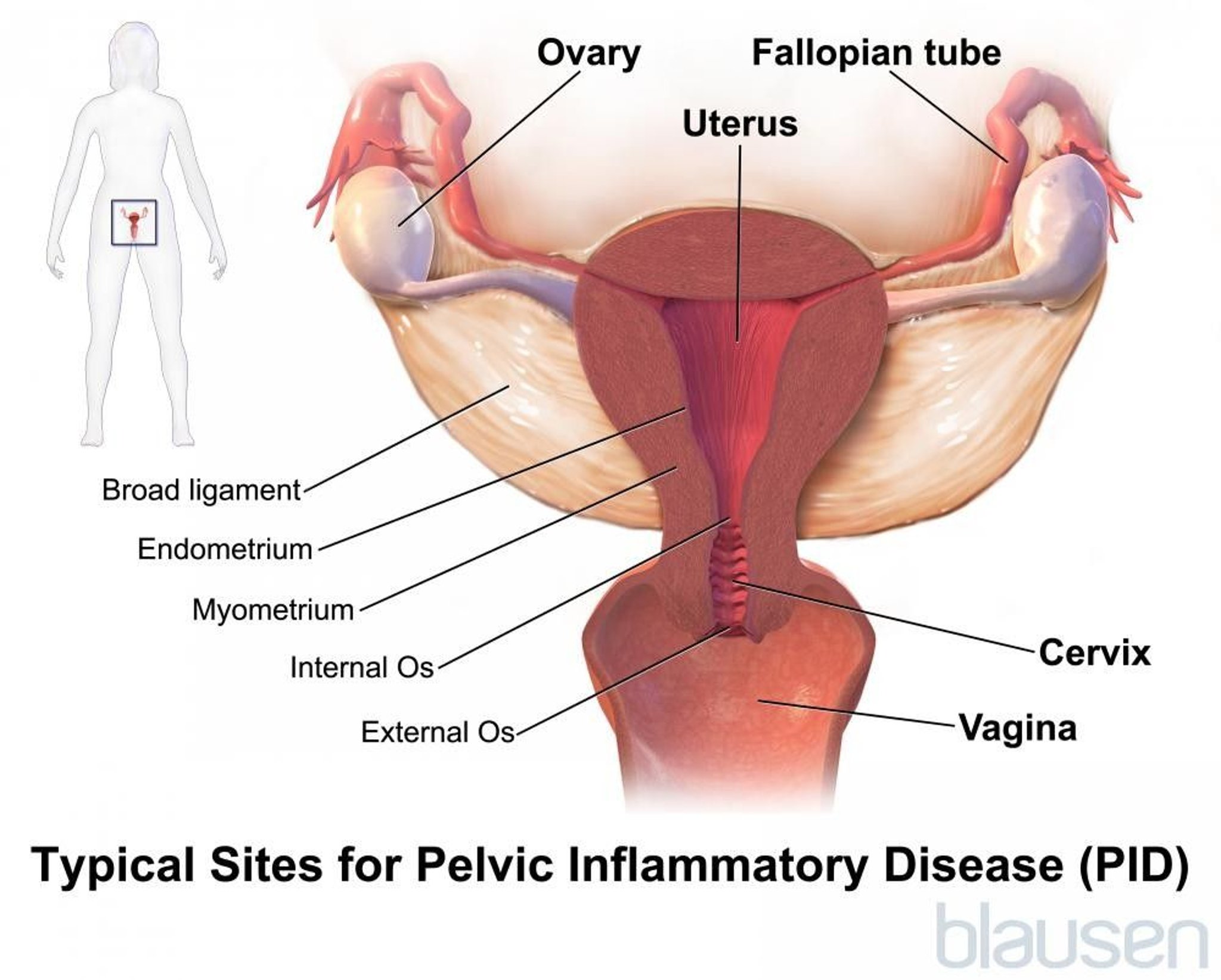
Pelvic inflammatory disease is an infection of the upper female reproductive organs (the cervix, uterus, fallopian tubes, and ovaries).
Pelvic inflammatory disease is often caused by a sexually transmitted infection.
Typically, women have pain in the lower abdomen, abnormal vaginal discharge, and sometimes fever or irregular vaginal bleeding.
The diagnosis is based on symptoms, analysis of secretions from the cervix, and sometimes blood tests or ultrasonography.
Treatment is with antibiotics.
Pelvic inflammatory disease may be an infection of the
Cervix, which is the lower, narrow part of the uterus that opens into the vagina (cervicitis)
Lining of the uterus (endometritis)
Fallopian tubes (salpingitis)
Ovaries (oophoritis)
Area around the ovaries and tubes (tubo-ovarian abscess)
A combination of the above

Pelvic inflammatory disease is the most common preventable cause of infertility in the United States. Many women who have had pelvic inflammatory disease have difficulty getting pregnant.
About one third of women who have had pelvic inflammatory disease develop the infection again.
Pelvic inflammatory disease usually occurs in sexually active women. It rarely affects girls before their first menstrual period (menarche) or women during pregnancy or after menopause. Risk factors are
Previous pelvic inflammatory disease
Other risk factors include
Sexual activity, especially in people younger than 35 years old
Multiple or new sex partners or a male partner who does not use a condom
Douching
Causes of Pelvic Inflammatory Disease
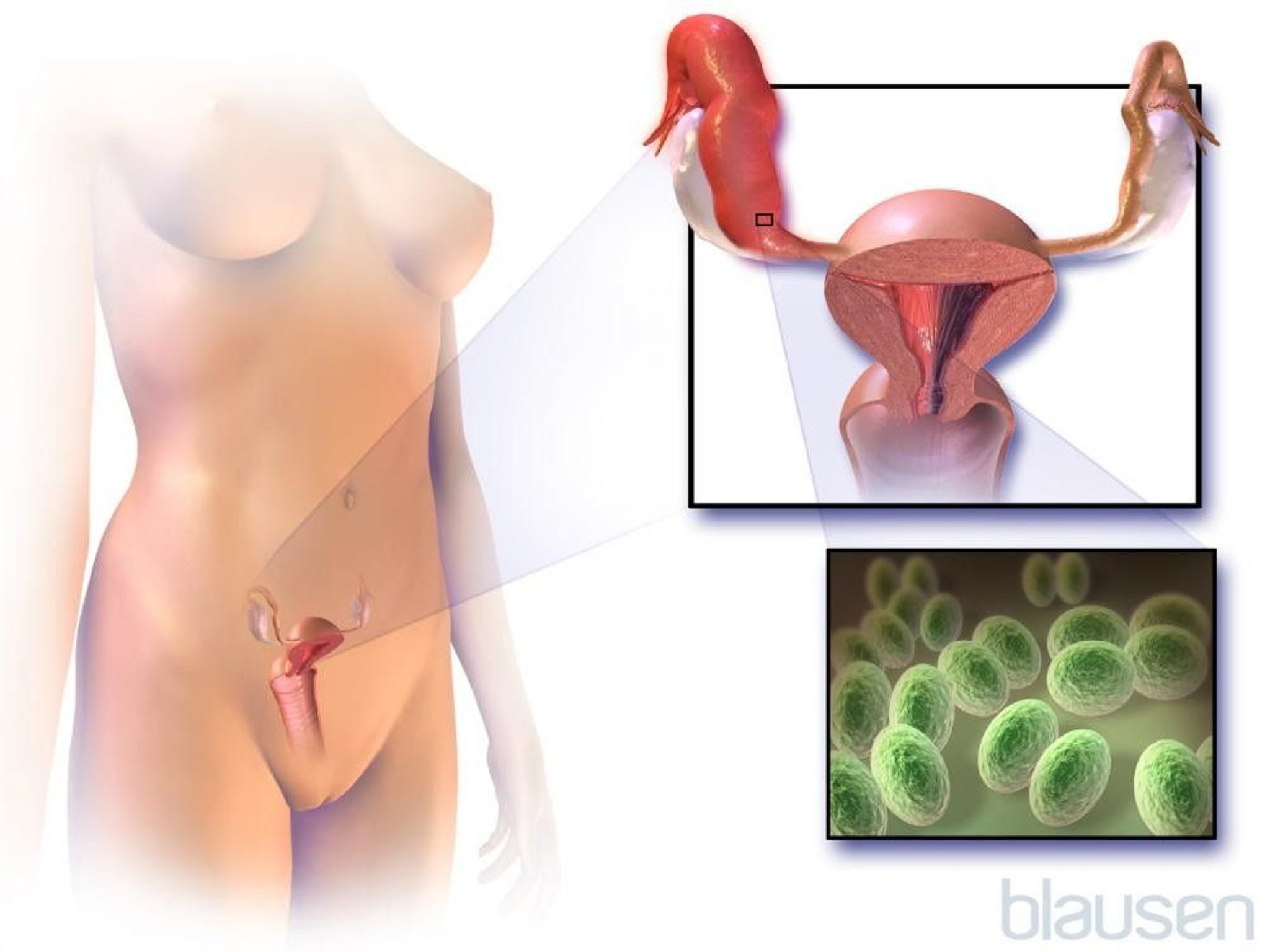
Pelvic inflammatory disease is usually caused by bacteria from the vagina. Most commonly, the bacteria are transmitted during sexual intercourse with a partner who has a sexually transmitted infection. The most common sexually transmitted bacteria are
These bacteria typically spread from the vagina to the cervix (the lower part of the uterus that opens into the vagina), where they cause infection (cervicitis). These infections may remain in the cervix or spread upward, causing pelvic inflammatory disease.

Pelvic inflammatory disease is also more common in women who have bacterial vaginosis. The bacteria that cause bacterial vaginosis normally reside in the vagina. They cause symptoms and spread to other organs only if they increase in number (overgrow). Whether bacterial vaginosis is sexually transmitted is unknown.
Less commonly, women are infected during a vaginal delivery, an abortion, or a medical procedure, such as dilation and curettage (D and C) or gynecologic surgery—when bacteria are introduced into the vagina or when bacteria that normally reside in the vagina are moved into the uterus.
Douching increases the risk of infection.
Did You Know...
|
Symptoms of Pelvic Inflammatory Disease
Symptoms of pelvic inflammatory disease commonly occur toward the end of the menstrual period or during the few days after it. For many women, the first symptom is mild to moderate pain (often aching) in the lower abdomen, which may be worse on one side. Other symptoms include irregular vaginal bleeding and a vaginal discharge, sometimes with a bad odor.
As the infection spreads, pain in the lower abdomen becomes increasingly severe and may be accompanied by a low-grade fever (usually below 102° F [38.9° C]) and nausea or vomiting. Later, the fever may become higher, and the discharge often becomes puslike and yellow-green. Women may have pain during sexual intercourse or urination.
The infection may be severe but cause mild or no symptoms. Symptoms due to gonorrhea tend to be more severe than those of chlamydia or infection due to Mycoplasma genitalium, which may not cause a discharge or any other noticeable symptoms.
Complications
Pelvic inflammatory disease can cause other problems, including the following:
Blocked fallopian tubes
Peritonitis (a serious abdominal infection)
Fitz-Hugh-Curtis syndrome (a serious infection of tissues around the liver)
An abscess (a collection of pus)
Adhesions (bands of scar tissue)
A pregnancy in a fallopian tube (tubal pregnancy)
Sometimes infected fallopian tubes become blocked. Blocked tubes may swell because fluid is trapped. Women may feel pressure or have chronic pain in the lower abdomen.
Peritonitis develops if the infection spreads to the membrane that lines the abdominal cavity and covers the abdominal organs. Peritonitis can cause sudden or gradual severe pain in the entire abdomen.
Fitz-Hugh-Curtis syndrome develops if infection of the fallopian tubes is due to gonorrhea or a chlamydia and it spreads to the tissues around the liver. Such an infection may cause pain in the upper right side of the abdomen. The pain resembles that of a gallbladder disorder or gallstones.
An abscess forms in the fallopian tubes or ovaries of about 15% of women who have infected fallopian tubes, particularly if they have had the infection a long time. An abscess sometimes ruptures, and pus spills into the pelvic cavity (causing peritonitis). A rupture causes severe pain in the lower abdomen, quickly followed by nausea, vomiting, and very low blood pressure (shock). The infection may spread to the bloodstream (a condition called sepsis) and can be fatal. It is a medical emergency.
Adhesions are abnormal bands of scar tissue. They can develop when pelvic inflammatory disease produces a puslike fluid. This fluid irritates tissues and causes bands of scar tissue to form in the reproductive organs or between organs in the abdomen. Infertility and chronic pelvic pain may result. The longer and more severe the inflammation and the more often it recurs, the higher the risk of infertility and other complications. The risk increases each time a woman develops the infection.
A tubal pregnancy (a type of ectopic pregnancy) is 6 to 10 times more likely to occur in women who have had pelvic inflammatory disease. In a tubal pregnancy, the fetus grows in a fallopian tube rather than in the uterus. This type of pregnancy threatens the life of the woman, and the fetus cannot survive.
Diagnosis of Pelvic Inflammatory Disease
A doctor's evaluation
Tests on a sample taken from the cervix
Sometimes ultrasonography or laparoscopy
Doctors suspect pelvic inflammatory disease if women have pain in the lower abdomen or if they have an unexplained discharge from the vagina, particularly if they are of childbearing age or if the discharge contains pus. A physical examination, including a pelvic examination, is done. Pain felt in the pelvic area during the pelvic examination supports the diagnosis.
A sample is usually taken from the cervix with a swab and tested to determine whether the woman has gonorrhea or chlamydia. Even if these tests do not detect gonorrhea or chlamydia, women may still have pelvic inflammatory disease.
Ultrasonography of the pelvis is done if pain prevents an adequate physical examination or if more information is needed. It can detect abscesses in the fallopian tubes or ovaries and a tubal pregnancy.
A pregnancy test is done to see whether the woman may have a tubal pregnancy, which could be the cause of the symptoms. Other symptoms and laboratory test results help confirm the diagnosis.
If the diagnosis is still uncertain or if the woman does not respond to treatment, the doctor may insert a viewing tube (laparoscope) through a small incision near the navel to view the inside of the abdomen and to obtain a sample of fluids for testing. This procedure can usually confirm or rule out pelvic inflammatory disease.
Treatment of Pelvic Inflammatory Disease
Antibiotics
If needed, drainage of an abscess
As soon as possible, antibiotics for gonorrhea and chlamydia are usually given by mouth or by injection into a muscle. Prompt treatment is needed to prevent serious complications. If needed, the antibiotics are changed after test results are available.
Most women are treated at home with antibiotics taken by mouth. However, hospitalization is usually necessary in the following situations:
The infection does not lessen within 72 hours.
The woman has severe symptoms or a high fever.
The woman may be pregnant.
An abscess is suspected.
The woman is vomiting and thus cannot take antibiotics by mouth at home.
Doctors cannot confirm the diagnosis of pelvic inflammatory disease and cannot rule out disorders that require surgery (such as appendicitis) as possible causes.
In the hospital, antibiotics are given intravenously.
Abscesses that persist despite treatment with antibiotics may be drained. Often, a needle can be used. It is inserted through a small incision in the skin, and an imaging test, such as ultrasonography or computed tomography (CT), is used to guide the needle into the abscess. A ruptured abscess requires emergency surgery.
Women should refrain from sexual activity until antibiotic therapy is completed and a doctor confirms that the infection is completely eliminated, even if symptoms disappear.
All recent sex partners should be tested for gonorrhea and chlamydia and, if needed, treated. If pelvic inflammatory disease is diagnosed and treated promptly, a full recovery is more likely.
Prevention of Pelvic Inflammatory Disease
Pelvic inflammatory disease is usually caused by sexually transmitted infections. Prevention includes safer sex practices and testing of people at risk for or with symptoms of these infections.
If used correctly, condoms can help prevent acquiring a sexually transmitted infection. To be effective, condoms must be used correctly each time a person has sex.






